- Home
- ENROLL in a program
- Nationwide On-Site 2 Day NFPT Workshop Program
- Express NFPT Certification Online Workshop Program
- Fundamentals of Personal Training
- Neuro-Functional R.O.M. Specialist
- Program Design For the Beginner Client –
- Lowering Cholesterol Through Progressive Resistance and Cardio Applications
- Nutrition Meal Planning for the Fat Loss Client:
- Personal Training: Making an Impact from day one
- Kettlebell Conditioning Specialist
- Asistencia en Español
- Calendar of Events
- Student Study Materials
- NFPT Express Workshop Study Files
- NFPT / GFE Nutrition Meal Planning for the Fat Loss Client Study Materials
- Program Design 1 Study Materials
- Lowering Cholesterol Through Progressive Resistance and Cardio Applications Study Materials
- Personal Training: Making an Impact from day one Study Materials
- CPR-AED
- Cart
02
JAN
2015
Squat, Press, Extend or Flex for Strong Legs and Healthy Knees
For decades the Leg Extension, Squat, Leg Press and Lunge have all been used by general fitness clients, rehab patients, and elite athletes alike without much on the side of specific research to help the fitness coach in determining which exercise to use or recommend for a specific goal or need. To understand the concepts and summaries of this article let’s start by taking an in-depth look at the internal components of the knee. As a trainer or coach you will probably hear over and over again about knee pain in all the people you will work with. Hence, a clear understanding of knee function and how the internal components affect such function is critical for programming, progressions, and when needed, regressions.
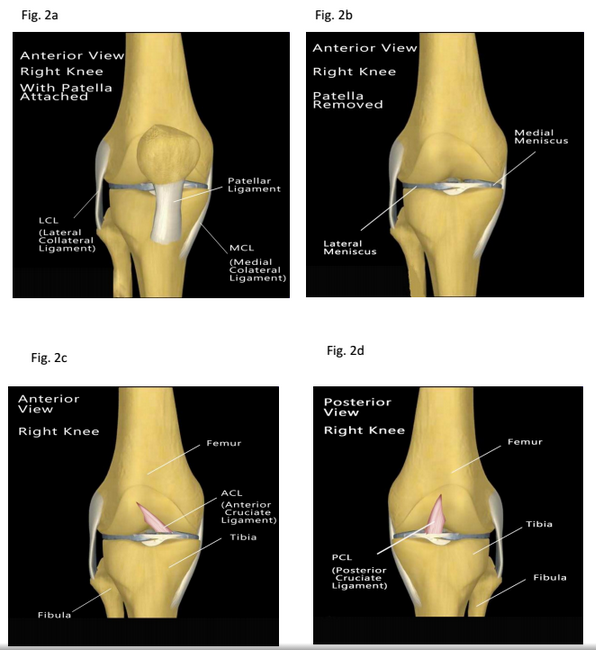
The knee, in its simplest description, is the union of the Femur, Tibia, and Fibula with a fourth and independent triangular bone that covers the front union, the Patella. Fig 1. Together, along with the structures that keep these bones aligned and able to provide us with flexible motion, are what we refer to as the Knee Joint. Technically named a synovial joint the knee is the largest and most complicated joint in the body and commonly referred to as a “hinge” joint for its linear and door like movement patterns.
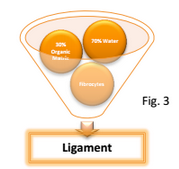 Ligaments, which connect one bone to another are composed of approximately 70% water and 30% organic matrix along with fibrocytes, the specific type of cells that make up tendons and ligaments (1,2). Without getting into chemistry and biology too deeply, the organic matrix is a combination of ground substance, (a combination of protein and carbohydrate complexes forming a gel like substance) and Collagen. Fig. 3.
To give further explanation, Fig. 4 illustrates the composition of the Organic Matrix into a classification of its internal composition. In Ligaments and Tendons, 90% of the Organic Substance is Collagen. Collagen comprises 25 to 30% of the protein in the body with at least
Ligaments, which connect one bone to another are composed of approximately 70% water and 30% organic matrix along with fibrocytes, the specific type of cells that make up tendons and ligaments (1,2). Without getting into chemistry and biology too deeply, the organic matrix is a combination of ground substance, (a combination of protein and carbohydrate complexes forming a gel like substance) and Collagen. Fig. 3.
To give further explanation, Fig. 4 illustrates the composition of the Organic Matrix into a classification of its internal composition. In Ligaments and Tendons, 90% of the Organic Substance is Collagen. Collagen comprises 25 to 30% of the protein in the body with at least 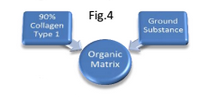 15 types of collagens currently known with more recent studies identifying more than 20 types! (2, 4) Collagen Fig.4 production in the body can vary from individual to individual with the aging process and genetics playing the biggest role in the ability to make adequate amounts for tissue repair and maintenance. In tendons and ligaments the type of Collagen found is called Type 1 which identifies its structural alignment, splice variants, and function when compared to the other many types of collagen in the body. (3, 4) Type 1 collagen fibers tend to be more rigid than Type 2. Hence, the ability to withstand the forces generated by movement and keep the bones they hold together without a daily injury.
Cartilage, which covers the end of all bones that touch each other is a bit different in its composition when compared to ligaments and tendons. When discussing the ligaments above and as will be discussed in part 2 of this series when we cover tendons, the cells that make up those structures are called “fibrocytes”. In Cartilage the cells are called Chondrocytes and the type of collagen is Type 2 vs. Type 1 in tendons and ligaments. (1,6,7)
Varieties of Cartilage
In the human body we can find three (3) types of cartilage.
1- Hyaline or Articular Cartilage is the main type of cartilage we will focus on with this article. This type of cartilage is most specifically found at the end of the long bones such as the Femur, Tibia, Fibula, Humerus, Radial, and Ulna but is also present in the sternum, ribs, and several other locations along the skeleton. It is bluish white in color, flexible, with low friction qualities that resist wear and tear and designed to bear and distribute loads. Therefore able to provide the cushioning needed for repetitive movements such as walking, running, jumping which are commonly referred to our “Activities of Daily Living” or “ADL’s, exercise, and sports.
2- Fibrocartilage , the second type of cartilage we will discuss. It can be temporarily found at bone fracture sites and is present in three major locations in the body. The intervertebral disks of the spine, covering the mandibular condyle in the temporomandibular joint, and in the Meniscus of the knee. Hence, the importance of identifying its composition and purpose.
3- Elastic Cartilage, the third type of cartilage is found I the pharyngotympanic tubes, epiglottis, and earlobes where the supportive tissue (cartilage) must possess elasticity. Hence, the name elastic cartilage.
Meniscus, is the final structure we will discuss in this article. (Fig 2b) The meniscus are two C shapes hybrid type of cartilage that act as the shock absorption system of the knee. The menisci help distribute stresses over a broad area of articular cartilage, absorb shock during dynamic loading, and help with joint lubrication. Unlike articular cartilage which is predominantly composed of Type 2 Collagen in the organic matrix, Menisci tissue is made up of the same coarse Type 1 Collagen Organic Matrix found in Tendons and Ligaments giving the meniscus the great tensile stiffness it exhibits. (9) Without the menisci, the daily stress of walking and the compounded effect of running, jumping, and weightlifting would be impossible. The menisci offer the additional protection to the articular cartilage covering the ends of the Femur and Tibia while simultaneously aiding in the lubrication of all the internal components of the knee.
15 types of collagens currently known with more recent studies identifying more than 20 types! (2, 4) Collagen Fig.4 production in the body can vary from individual to individual with the aging process and genetics playing the biggest role in the ability to make adequate amounts for tissue repair and maintenance. In tendons and ligaments the type of Collagen found is called Type 1 which identifies its structural alignment, splice variants, and function when compared to the other many types of collagen in the body. (3, 4) Type 1 collagen fibers tend to be more rigid than Type 2. Hence, the ability to withstand the forces generated by movement and keep the bones they hold together without a daily injury.
Cartilage, which covers the end of all bones that touch each other is a bit different in its composition when compared to ligaments and tendons. When discussing the ligaments above and as will be discussed in part 2 of this series when we cover tendons, the cells that make up those structures are called “fibrocytes”. In Cartilage the cells are called Chondrocytes and the type of collagen is Type 2 vs. Type 1 in tendons and ligaments. (1,6,7)
Varieties of Cartilage
In the human body we can find three (3) types of cartilage.
1- Hyaline or Articular Cartilage is the main type of cartilage we will focus on with this article. This type of cartilage is most specifically found at the end of the long bones such as the Femur, Tibia, Fibula, Humerus, Radial, and Ulna but is also present in the sternum, ribs, and several other locations along the skeleton. It is bluish white in color, flexible, with low friction qualities that resist wear and tear and designed to bear and distribute loads. Therefore able to provide the cushioning needed for repetitive movements such as walking, running, jumping which are commonly referred to our “Activities of Daily Living” or “ADL’s, exercise, and sports.
2- Fibrocartilage , the second type of cartilage we will discuss. It can be temporarily found at bone fracture sites and is present in three major locations in the body. The intervertebral disks of the spine, covering the mandibular condyle in the temporomandibular joint, and in the Meniscus of the knee. Hence, the importance of identifying its composition and purpose.
3- Elastic Cartilage, the third type of cartilage is found I the pharyngotympanic tubes, epiglottis, and earlobes where the supportive tissue (cartilage) must possess elasticity. Hence, the name elastic cartilage.
Meniscus, is the final structure we will discuss in this article. (Fig 2b) The meniscus are two C shapes hybrid type of cartilage that act as the shock absorption system of the knee. The menisci help distribute stresses over a broad area of articular cartilage, absorb shock during dynamic loading, and help with joint lubrication. Unlike articular cartilage which is predominantly composed of Type 2 Collagen in the organic matrix, Menisci tissue is made up of the same coarse Type 1 Collagen Organic Matrix found in Tendons and Ligaments giving the meniscus the great tensile stiffness it exhibits. (9) Without the menisci, the daily stress of walking and the compounded effect of running, jumping, and weightlifting would be impossible. The menisci offer the additional protection to the articular cartilage covering the ends of the Femur and Tibia while simultaneously aiding in the lubrication of all the internal components of the knee.
Ligaments, which connect one bone to another are composed of approximately 70% water and 30% organic matrix along with fibrocytes, the specific type of cells that make up tendons and ligaments (1,2). Without getting into chemistry and biology too deeply, the organic matrix is a combination of ground substance, (a combination of protein and carbohydrate complexes forming a gel like substance) and Collagen. Fig. 3.
To give further explanation, Fig. 4 illustrates the composition of the Organic Matrix into a classification of its internal composition. In Ligaments and Tendons, 90% of the Organic Substance is Collagen. Collagen comprises 25 to 30% of the protein in the body with at least 15 types of collagens currently known with more recent studies identifying more than 20 types! (2, 4) Collagen Fig.4 production in the body can vary from individual to individual with the aging process and genetics playing the biggest role in the ability to make adequate amounts for tissue repair and maintenance. In tendons and ligaments the type of Collagen found is called Type 1 which identifies its structural alignment, splice variants, and function when compared to the other many types of collagen in the body. (3, 4) Type 1 collagen fibers tend to be more rigid than Type 2. Hence, the ability to withstand the forces generated by movement and keep the bones they hold together without a daily injury.
Cartilage, which covers the end of all bones that touch each other is a bit different in its composition when compared to ligaments and tendons. When discussing the ligaments above and as will be discussed in part 2 of this series when we cover tendons, the cells that make up those structures are called “fibrocytes”. In Cartilage the cells are called Chondrocytes and the type of collagen is Type 2 vs. Type 1 in tendons and ligaments. (1,6,7)
Varieties of Cartilage
In the human body we can find three (3) types of cartilage.
1- Hyaline or Articular Cartilage is the main type of cartilage we will focus on with this article. This type of cartilage is most specifically found at the end of the long bones such as the Femur, Tibia, Fibula, Humerus, Radial, and Ulna but is also present in the sternum, ribs, and several other locations along the skeleton. It is bluish white in color, flexible, with low friction qualities that resist wear and tear and designed to bear and distribute loads. Therefore able to provide the cushioning needed for repetitive movements such as walking, running, jumping which are commonly referred to our “Activities of Daily Living” or “ADL’s, exercise, and sports.
2- Fibrocartilage , the second type of cartilage we will discuss. It can be temporarily found at bone fracture sites and is present in three major locations in the body. The intervertebral disks of the spine, covering the mandibular condyle in the temporomandibular joint, and in the Meniscus of the knee. Hence, the importance of identifying its composition and purpose.
3- Elastic Cartilage, the third type of cartilage is found I the pharyngotympanic tubes, epiglottis, and earlobes where the supportive tissue (cartilage) must possess elasticity. Hence, the name elastic cartilage.
Meniscus, is the final structure we will discuss in this article. (Fig 2b) The meniscus are two C shapes hybrid type of cartilage that act as the shock absorption system of the knee. The menisci help distribute stresses over a broad area of articular cartilage, absorb shock during dynamic loading, and help with joint lubrication. Unlike articular cartilage which is predominantly composed of Type 2 Collagen in the organic matrix, Menisci tissue is made up of the same coarse Type 1 Collagen Organic Matrix found in Tendons and Ligaments giving the meniscus the great tensile stiffness it exhibits. (9) Without the menisci, the daily stress of walking and the compounded effect of running, jumping, and weightlifting would be impossible. The menisci offer the additional protection to the articular cartilage covering the ends of the Femur and Tibia while simultaneously aiding in the lubrication of all the internal components of the knee.
5 Comments
It’s hard to find knowledgeable people for this subject, however, you seem like you know what you’re talking about!
Thanks
Your welcome. We look forward to having in one of our workshops.
Oh my goodness! Awesome article dude! Thank you so much, However I am encountering issues with your RSS.
I don’t know why I cannot join it. Is there anybody else getting similar RSS issues?
Anybody who knows the solution will you kindly respond? Thanks!!
Pingback: Google
Hello to all, the contents present at this website are actually awesome for people
experience, well, keep up the nice work fellows.